How MSOs Lower Medical Costs and Turn a Profit

In yesterday’s Bloomberg Businessweek, John Tozzi highlights a not-so-new business strategy that has some investors’ attention and might just help taxpayers if it is both successful and the opportunity for the business diminishes over time (except that won’t help the investors).
One Health-Care Company’s Audacious Plan to Lower Costs—and Still Turn a Profit

Here’s the gist: primary care providers (PCPs) engage high risk Medicare beneficiaries on a routine basis for low level office visits and to monitor health and provide preventive care (nickels, nickels, …, nickels) and as a result those same high risk patients have fewer hospitalizations over time and as a group (saving dollars, dollars, …, dollars) creating a savings on the overall cost of care over time, for which the PCPs have taken substantial financial risk (see: FRG’s article CMS Provider Incentive Plans (PIP) Regulations and Stop Loss Reinsurance Requirements) and therefore can retain as earnings (read: keep the change). Of course, it can go the other way too, but never mind that for now.
The backdrop is this: hospital emergency departments have seen their fair share of Medicare patients and then some. According to the American Hospital Association, “about 42 percent of the typical hospital’s volume” is Medicare patients. Thus, specific health clinics, such as Oak Street Health, Inc., have devised a new approach to this ongoing issue with the intention of “reinvent[ing] care for Medicare patients with low incomes and chronic health problems.”
This, of course, makes sense demographically and prognostically. In 2021, we are 66 years from the middle of the baby boom. And the link between age and morbidity is well established, Oscar Swan notwithstanding. The baby boom has concentrated the need for medical services to the elderly, most of which are eligible for Medicare and many of which are in fact dually eligible due to socioeconomic status.
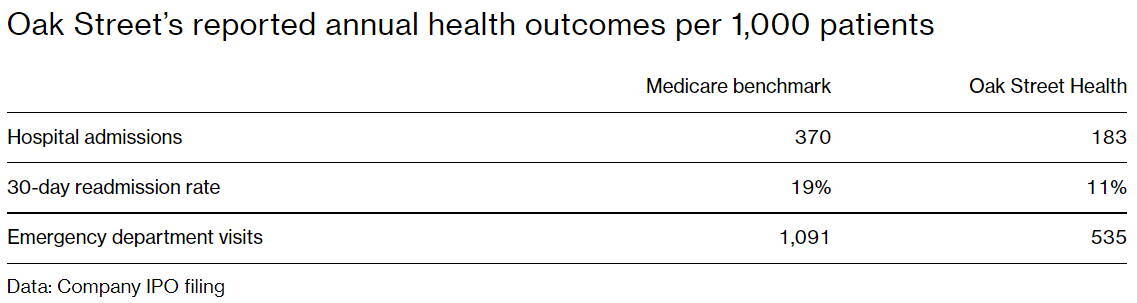
The hypothesis: if Medicare patients receive higher amounts of primary care, then the number of costly hospital admissions decreases. So far, this hypothesis has proven truthful. Oak Street says its “patients go to hospitals about half as often as the general Medicare population.”
Oak Street plans to see its more vulnerable patients every few weeks and its healthier patients every few months. With these frequent checkups in addition to preventive screenings, meetings with social workers, and free rides to their clinics, Oak Street foresees a reduction in its patients’ medical costs.
Efficient, Fully Accountable Care
Of course, Oak Street can only operate this way in part by changing the way it is compensated. The typical fee-for-service model where payment is generated by a test, procedure, or visit “directs too much time and money to expensive, needless services, while other valuable care—such as preventive screening—is neglected.”
This new arrangement allows Oak Street to receive a monthly per-patient fee from Medicare, and “the plans then pass most of that fee on to Oak Street for patients who sign up.” This renders the clinic responsible for those patients’ total cost of care, and for Oak Street to turn a profit, the Medicare payment must outweigh that of its members’ medical costs.
In its Risk Adjusted Revenue model, Medicare makes a greater allowance for medical cost for patients with documented chronic conditions (i.e. sicker patients) to eliminate the cherry picking of healthier members. When the money to cover these expectations flows through a health plan to a provider organization taking full risk, like Oak Street, the opportunity to manage those medical needs by working toward improving their overall health with more wellness visits and less costly visits emerges.
Oak Street Health, Inc. has more than 90 centers in 15 states with plans for more to come. Currently, “the company is valued at $14 billion,” and several other upstarts and industry leaders are moving in this strategic direction.
Turning a profit, maybe?
Although highly valued, questions remain as to Oak Street’s ability to turn a profit. Its expansion investments are hurting the clinic’s bottom line. And others debate this new strategy’s efficacy altogether. Of course, difficulty reaching profitability in provider network integration is not new. Echoes of PhyCor come to mind, but the novelty of global capitation sets it apart. PhyCor tried to integrate physician practice clinical operations before the Internet, at the dawn of electronic medical records and before much in the way of practice integration technologies were possible, and most notably before capitated payment models had escaped the Golden State.
Clearly, Oak Street and others have an opportunity under current arrangements to create a savings and retain a profit. In the short run, if they can lower medical costs, then they keep the change, so to speak, but if pressure on total Medicare spending continues to rise, then we should expect to see a long-term decline in risk adjustment base rates which will transfer those savings to tax payers. When will that be is anyone’s guess.
Read the full article: One Health-Care Company’s Audacious Plan to Lower Costs—and Still Turn a Profit