
The Centers for Medicare and Medicaid services (CMS) implemented the Risk Adjustment Payment System (RAPS) program as a way to determine a Medicare Advantage member’s premium on a prospective basis. While RAPS has gone through several changes over the years, the goal is to pay MA and Prescription Drug Plans (PDPs) accurately and fairly by adjusting payment for members based on demographics and health status.
Understanding Medicare Risk Adjustment Best Practices
To properly estimate what dollars are required on a member by member basis, over 17,000 ICD-9s (and ICD-10s) have been analyzed and nearly 3,000 of those have been cross-walked to 90+ Hierarchical Condition Categories (HCC). Each of the HCCs have a value attached to them payment model. When those values are added together with the age/sex and additional factors, the sum results in the Medicare Risk Adjustment (MRA) score.
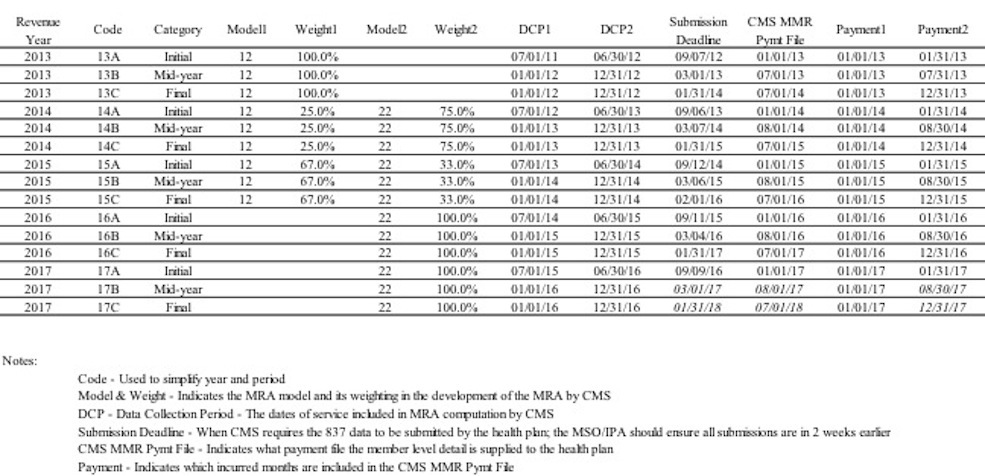
“Prospective-based” means that prior year ICD-9s generate next year’s revenue. In other words, a member’s diagnosis codes recorded in 2015 will result in the MA premium for 2016. There are three points in time when CMS “freezes” the claim and encounter data it receives in to re-calibrate the members MRA score. There is the initial, the mid-year recon and final recon. Each is based on information submitted by the MA health plan before CMS’ deadlines. These deadlines can be found in the table below.
Health Plan Claims Auditing
Health plans and providers may conduct a few claim audits to ensure all correctly documented diagnosis codes have been submitted. The audit may be retrospective, look into prior years to capture lost opportunity before the final MRA reconciliation, and prospective, audit current year coding to identify undercoded and overcoded diagnosis codes for next year’s premium.
Retrospective audits are generally performed by a third party if the provider does not employ a Certified Practice Coder (CPC) so the third party can offer an unbiased opinion of the providers documentation and coding efficiency and accuracy. This allows the provider to make corrections, not to the prior member visits, to his/her documentation for future visits.
Prospective audit initiatives can be conducted by the provider, the health plan or even a third party. Prospective activity really starts with the first appointment of the new year. The provider should review the active HCCs an MA member has had over the last couple of years. MA members should be seen at least 4 times per year for a healthy member and depending on the member’s health status perhaps over 10 times a year. The average MA member should be seen around 6 to 8 times. This requires frequent outreach (letters, phone calls, etc.) by the provider’s team, member education, perhaps in home assessments.
At the first visit for the year, the provider or PA should conduct a thorough Health Risk Assessment (HRA) to ensure all prior health issues have been accurately documented and assessed. Additionally, the provider asks questions to identify new issues that may have surfaced. The provider must ask questions and document, document, document. Is the condition controlled, uncontrolled, stable, worsening, asymptomatic? Document lab and test findings in the progress note. Watch for conflicting data in the progress notes.
Over time the coding habits a provider develops for his/her MA members, should be duplicated for all members—traditional Medicare FFS, commercial, Medicaid, etc. When members decide to move into MA, there will be a higher probability that the premium from CMS will more accurately reflect the medical conditions thereby allowing aligning the premium with the corresponding medical expense immediately.
Key Dates (click table to enlarge)
Want a tool to help you calculate MRA scores? Try the new MRA Calculator





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Leave A Comment